Welcome to this in-depth case study walkthrough by Dr. Gaurav, a board-certified hair transplant surgeon. In this video, he unpacks Case #344, a corrective hair transplant performed on a patient from Melbourne who’d previously undergone an underwhelming procedure abroad. Unlike typical “before-and-after” reels, this isn’t just about aesthetics. It’s about realistic expectations, surgical ethics, and why how many grafts matters far less than how well they’re placed. Whether you’re researching transplants or recovering from one, this breakdown cuts through marketing noise and gets real about what actually works and why.
Background
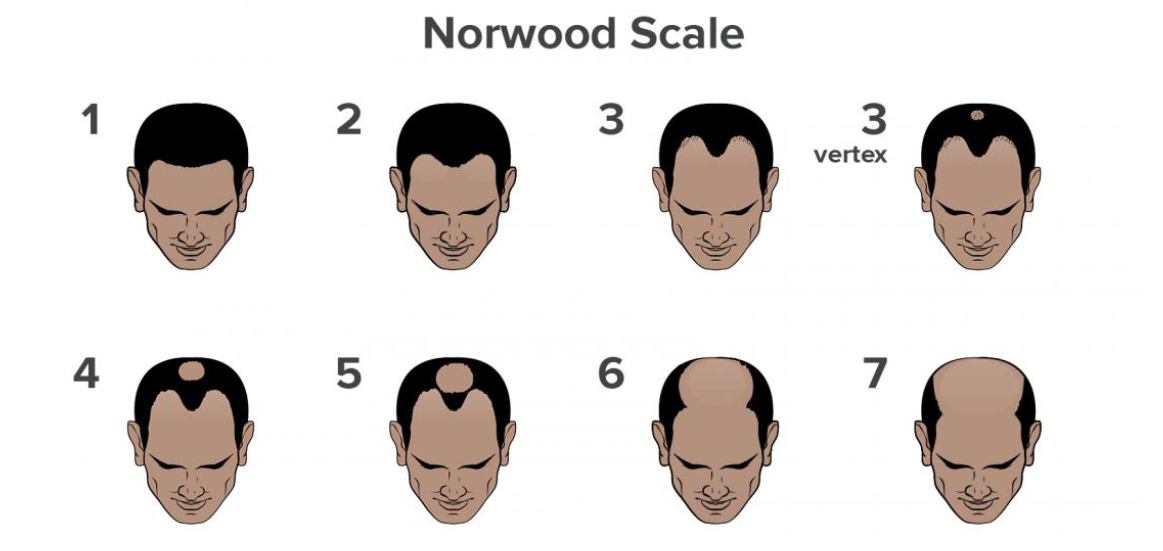
Hair transplant tourism has surged globally, especially among patients from countries like Australia, the UK, and the US seeking lower-cost procedures abroad. But as Dr. Gaurav explains, many overseas clinics operate with limited surgical teams, often relying on technicians rather than experienced surgeons for critical steps like graft extraction and placement. This leads to suboptimal outcomes: sparse density, poor angle control, unnatural hairlines, and wasted donor supply. Case #344 exemplifies this a Grade 4 Norwood classification (significant frontal and mid-scalp recession with preserved crown) where only a minimal number of grafts were placed during the initial surgery in Melbourne. The patient continued medical therapy (minoxidil + biotin) remotely but needed structural correction, not just more hair, but strategically re-engineered coverage. Crucially, he returned to India every 6–7 months for follow-ups and adjunct therapies like GFC (Growth Factor Concentrate) therapy. Platelet-rich plasma–derived treatment administered on the same day as his corrective transplant to boost graft survival and accelerate healing.
Key Insight #1: Corrective Surgery ≠ Just Adding More Grafts
A corrective hair transplant isn’t about stacking grafts on top of old ones, it’s about rebuilding architecture. In Case #344, the prior surgery created patchy, low-density zones and an overly linear hairline. Dr. Gaurav didn’t simply “fill gaps.” Instead, he performed a density-driven revision: placing finer, single-hair grafts at the front for softness; using 2–3 hair units behind for transition; and layering denser 3–4 hair grafts in the mid-scalp to restore optical fullness. Critically, he preserved untouched donor tissue because overharvesting in corrective cases risks future options. This approach reflects what he calls “futuristic transplantation”: planning not just for today’s coverage, but for aging, potential thinning, and long-term aesthetic harmony. It’s surgical foresight not just technical execution.
Key Insight #2: Graft Count Is Meaningless Without Context
Dr. Gaurav bluntly calls out misleading clinic marketing: “Unlimited grafts,” “5,000+ grafts guaranteed,” or price-per-graft models are red flags especially for advanced baldness (Grade 4+). Why? Because biological limits apply. A Grade 4 scalp may require up to ~4,500 grafts max for natural, non-stretched coverage but only if donor supply, skin elasticity, and blood supply allow it. Pushing beyond that causes visible scarring, poor growth, or “doll’s hair” density. Worse, confusing grafts (the implanted unit) with follicular units (natural groupings of 1- 4 hairs) misleads patients. A clinic quoting “3,000 follicles” might mean just 1,800 actual grafts and no patient can verify counts intraoperatively.
Key Insight #3: Medical Support Isn’t Optional — It’s Foundational
Even with perfect surgery, grafts need biological support to thrive especially in revision cases where scar tissue and compromised blood flow exist. That’s why GFC therapy was timed on the day of transplant: injected into recipient sites to deliver concentrated growth factors (VEGF, PDGF, IGF-1) that reduce inflammation, stimulate angiogenesis, and extend the anagen (growth) phase. Combined with ongoing minoxidil and biotin maintained consistently despite geographic distance. This created a synergistic environment for retention and maturation. For international patients, continuity of care isn’t logistical; it’s clinical. Dr. Gaurav’s model blending in-person surgical precision with remote medical stewardship proves that world-class outcomes depend on systems, not just skill.
Conclusion
Hair Transplant Case Result 344 is a masterclass in responsible hair restoration: no hype, no shortcuts, just layered expertise. It reminds us that hair loss isn’t solved by volume alone. It’s solved by vision (understanding pattern progression), integrity (rejecting unrealistic graft promises), and integration (blending surgery with science-backed medical therapy). If you’re considering a transplant, especially after a prior procedure, prioritize surgeons who document real revisions (not just ideal candidates), explain why certain techniques suit your grade and goals, and treat you as a long-term partner, not a one-time client. Spend time on our website, watch their case studies, read patient journeys not just testimonials. And if a clinic leads with numbers over nuance? Walk away. Because in hair restoration, the most powerful metric isn’t graft count. it’s confidence in the craft. Keep learning, keep asking questions, and remember: great results grow slowly but they start with the right foundation.